Les risques de long-terme pour les patients post-Covid-19 et les implications pour la souscription en réassurance
8 septembre 2020

(Article en anglais) Those who have recovered from the COVID-19 virus remain vulnerable to long-term after-effects which increase morbidity and heighten mortality risk. While experience with other Coronavirus outbreaks provides insight into the post-COVID-19 health threats, including psychological issues, patients should be monitored on an ongoing basis.
The Long-Term Health Risks for Post-COVID-19 Patients
& the Implications for Reinsurance Underwriting
In this article, Medical and Underwriting professionals at SCOR Global Life take a detailed look at the types of health risks, and the implications for underwriting reinsurance, in the post-COVID-19 landscape.
Part 1: Post-COVID-19: Predicting the Future by Looking at the Past
Individuals who survive serious and critical illness often manifest after-effects resulting in increased future morbidity and mortality risk. Survivors of severe COVID-19 are also likely to have excess morbidity and risk of increased mortality. Predicting long-term outcomes of COVID-19 survivors is especially difficult as this illness has been identified for less than a year.
In addition, the causative SARS-CoV-2 virus is unique and has been challenging on several fronts. However, past experiences provide us with some clues as to expected outcomes. Pertinent data can be obtained from several sources:
- Studies on post-intensive care syndrome (PICS), often as a result of Acute Respiratory Distress Syndrome (ARDS);
- The two prior major coronavirus outbreaks, Severe Acute Respiratory Syndrome (SARS) and Middle Eastern Respiratory Syndrome (MERS); and
- Integrating the information that has been learned from COVID-19 thus far.
Post-Intensive Care Syndrome (PICS)
First, a little about the history of intensive care units (ICUs). ICUs began in the 1950s with the use of intermittent positive pressure ventilators (IPPV) as a treatment for polio. Initially, outcomes were measured simply as survival vs. death. It was not until the 1970s that the first post-ICU outcome study was published. The first post-ICU clinic was established in the 1990s.
In 1999 it was noted that cognitive impairment following ARDS persisted in 30% of survivors at one year. Neuromuscular dysfunction was first noted in 1984, and now ~50% of post-ICU patients have some form of polyneuropathy. Recent studies have indicated that acute kidney injury (AKI) is a marker for poor prognosis post-ICU.
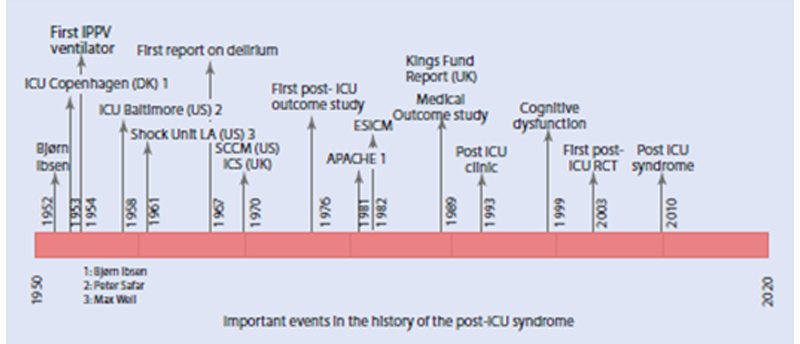
Source: Preiser, Jean-Charles, Margaret S. Herridge, and Elie Azoulay, eds. Post-Intensive Care Syndrome. Springer, 2020
There are different types of critical illness that can occur post-ICU, and although there is some inconsistency in the literature, they fall into two main categories:
- Chronic critical illness, which is secondary to the primary reason for the initial ICU stay, i.e., prolonged ventilation secondary to profound weakness as a result of ALS (Lou Gehrig’s Disease). In this type, the reason for which the person entered the ICU cannot be cured.
- Persistent critical illness, in which the issues are no longer directly attributable to the reason that one entered the ICU in the first place. These conditions may occur in anyone admitted to the ICU for an extended period (including severely ill COVID-19 patients):
- Poor nutrition
- Endocrinopathies
- Infections - often secondary to invasive monitoring and procedures
- Neuromuscular weakness
- Cognitive issues and brain dysfunction
- Mood, anxiety, PTSD.
SARS
The SARS outbreak occurred in 2002-2003, with 8,096 cases and 774 deaths reported, resulting in a 9.6% mortality rate. Large numbers of healthcare workers were affected, but few children were. Asymptomatic infection was infrequent. The lungs and the GI tract were primarily affected with ACE2 receptors acting as the means of cellular entry (the same receptor used by SARS-CoV-2). The two pathogenic mechanisms of this disease were the direct lytic effect on the host cells as well as the indirect effect from the host immune response.
MERS
The MERS outbreak has been ongoing since 2012, with 2,494 cases reported in 27 countries and 858 deaths, resulting in a 34% mortality rate. Healthcare outbreaks have been frequent, with rare pediatric cases and evidence of poor human-to-human transmission.
COVID-19
SARS-CoV-2 appears to have four mechanisms of action:
- Directly attacking organs via their ACE2 receptor
- Indirectly attacking organs by way of collateral damage from the cytokine storm
- Indirectly causing damage to organs secondary to blood clots
- Indirectly causing damage from low blood and tissue oxygen levels.
During the course of the illness, damage may also occur from mechanical ventilation, secondary infections and/or other treatments. Future morbidity and mortality risk will likely depend on the organs affected and the extent of the damage.
Pulmonary Impact
The majority of symptomatic infections affect the pulmonary system. The lungs in COVID-19 pneumonia show damage to alveoli and pulmonary capillaries, which are the two sides of the interface where oxygen and carbon dioxide are exchanged during breathing.
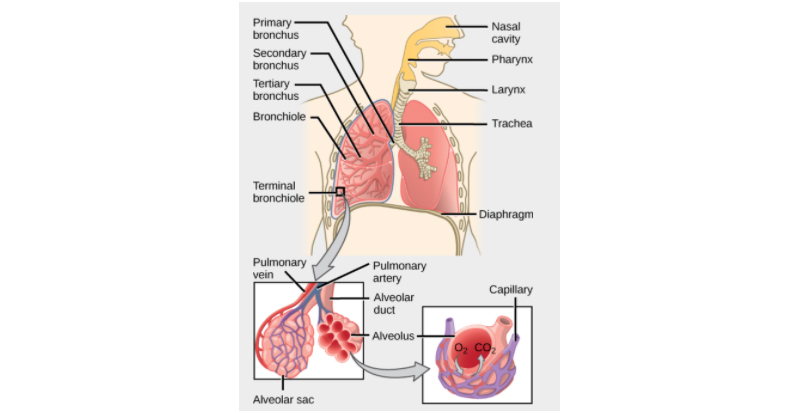
Source: CNX OpenStax - http://cnx.org/contents/GFy_h8cu@10.53:rZudN6XP@2/Introduction,
CC BY 4.0, https://commons.wikimedia.org/w/index.php?curid=49935216
Severe damage to this interface leads to hypoxia. If hypoxia progresses unchecked, there may be a need for supplemental oxygen and eventually artificial ventilation. For some, this severe lung damage results in death. But most have a brief illness with full resolution of normal function.
There are some, and right now we do not have accurate numbers, in whom there is more permanent damage with fibrosis and scarring of lung tissue. Two long-term studies looked at SARS survivors at seven years and at 15 years after illness and found that, although there still may be radiologic evidence of scarring and fibrosis, pulmonary function tests return to between mildly impaired (>80% expected function) and normal function in the vast majority of patients.
Many studies indicate that improvements began approximately six months after recovery. ARDS studies point toward similar functional recovery at five years, with younger patients recovering more function than older patients.
Clearly we have no long-term COVID-19 recovery studies, but most cases of ARDS and previous severe SARS (a similar coronavirus) patients have recovered lung function to near normal with time, and barring any new information, it is not unrealistic to expect that most COVID-19 survivors will do the same.
Cardiovascular Concerns
Another concern with severe COVID-19 is the effect on the cardiovascular system. Having cardiovascular disease increases the risk of developing severe COVID-19, and having COVID-19 can also induce cardiac complications in previously healthy individuals.
Complications that have been seen thus far include acute myocardial infarction, myocarditis, heart failure, cardiomyopathy, arrhythmias, shock and cardiac arrest as well as strokes and venous thromboembolic events. If the heart was damaged/involved during acute infection with COVID-19, the subsequent risks of those impairments exist, and necessary medical follow-up is essential.
Two recent studies on COVID-19 patients, one conducted in China and the other in Germany, demonstrate that cardiac involvement can be found in patients who did not have any indication of cardiac trouble during their acute illness. Both studies found evidence of myocardial edema and scarring at a median of two to three months post-infection. These were small studies (26 and 100 patients), but most had mild to moderate illness, and 18 were asymptomatic.
The first found 58% and the second noted that 78% of COVID-19 patients had magnetic resonance imaging (MRI) evidence of myocardial edema (indicating acute inflammation) and/or fibrosis or scarring. A few autopsy studies have found evidence of SARS-CoV-2 virus present in the heart in COVID patients who did not fulfil clinical criteria for myocarditis. Undeniably, these patients had severe infection resulting in death. There is a definite need for further studies regarding these cardiac findings, and the long-term effect of COVID19 on the cardiovascular system is not yet known.
Acute Kidney Injury
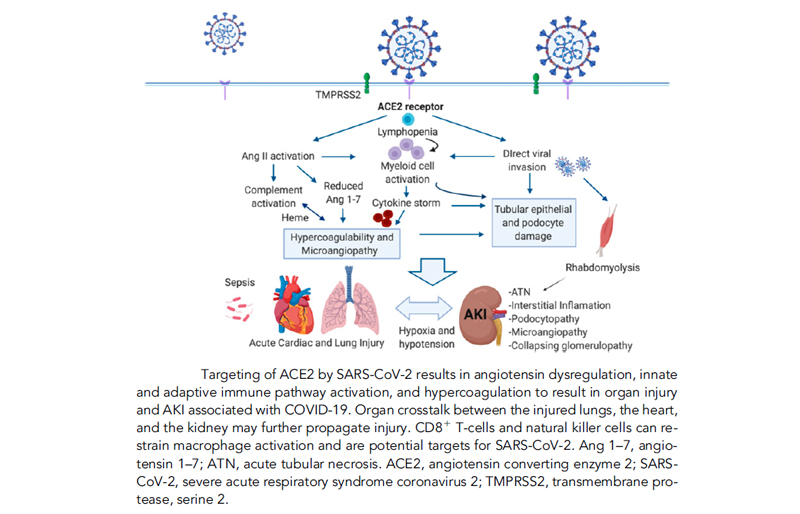
A large observational study in NYC on COVID-19 hospitalized patients showed that acute kidney injury (AKI) occurred in 37% of the patients. Independent risk factors for this include older age, hypertension, cardiovascular disease, diabetes, vasopressor use, need for artificial ventilation and black race. AKI occurs early and frequently among hospitalized patients and is associated with poor prognosis. There is limited knowledge on the pathophysiology of kidney injury, but it appears to be an interplay of virus-mediated injury, cytokine storm and complement pathway activation, hypercoagulation and known risk factors (diabetes, hypertension, etc.).
For those who survive, long term effects of AKI are unknown. Further studies are needed in this area.
Batlle, Daniel, et al. "Acute kidney injury in COVID-19: emerging evidence of a distinct pathophysiology." Journal of the American Society of Nephrology (2020).
Hypercoagulability and thrombosis
Hypercoagulability and thrombosis are a common occurrence in all ICU patients, but they appear to be more prevalent in COVID-19. With experience, healthcare providers have refined the care and prevention of thrombosis in COVID-19 patients, but it is still a prominent feature of the disease. A high incidence of deep vein thrombosis (DVTs) and pulmonary emboli (PEs) has been observed, with the incidence highest in ICU patient > non-ICU patients > outpatients.
Arterial thrombosis, including myocardial infarctions, central nervous system clots such as strokes and limb thrombosis have all been reported. Microvascular thrombosis has been noted on several autopsy studies as well. If a patient has been affected by these abnormal clotting issues, they need professional management and follow-up. The duration of increased risk of clotting in recovering COVID-19 patients remains unclear. The recommendation from several professional societies suggests risk stratifying patients and proceeding with prophylactic anticoagulation if indicated.
Neurologic Complications
In addition to strokes, other neurologic complications of COVID-19 have been reported. Anosmia, headache and severe fatigue are prominent non-respiratory symptoms during the acute phase of the illness. Other neurologic complications seen in viral infections, including COVID-19, are: viral meningitis, encephalitis, postinfectious acute disseminated encephalomyelitis (ADEM), Guillain-Barre syndrome, myositis and acute necrotizing encephalopathy. With any of these conditions appropriate medical follow-up is required, and a risk of future morbidity and mortality is expected.
Neuro-psychiatric Symptoms
Finally, neuro-psychiatric symptoms have been observed and studied in SARS and MERS survivors. There has been a significant increased incidence of post-traumatic stress disorder (PTSD), anxiety, depression and chronic fatigue syndrome following other coronavirus illnesses, and it would also be likely to occur in COVID-19 survivors.
Several different studies have given approximately the same percentages of chronic fatigue syndrome ~40% for both SARS and MERS up to four years after the acute infection. Also, both SARS and MERS survivors have an increase in psychiatric illness, including depression and PTSD.
Lam found at a 3.5-year follow up that 40% of the survivors had active psychiatric illness, whereas before contracting SARS, only 3.3% had a history of psychiatric disorders. While it is very difficult to sort the contribution of the stress and anxiety of being in an ICU from the damage done by the illness itself, it is evident that a high amount of morbidity remains years after other coronavirus infections. Patients with psychiatric illness are often less diligent with compliance and follow-up with other medical problems as well, so potentially increased mortality risk is possible.
Looking Forward
With every new day, medical professionals are learning better ways to manage COVID-19 and all its comorbidities. Many collaborations and databases have been established to share knowledge on the pathophysiology, epidemiology, treatment, and prognosis. It is beyond the scope of this article to discuss vaccines, which provide us with the hope of ending this pandemic. But, even when the pandemic is under control, there will still be COVID-19 survivors living with the complications and residuals of the disease. As such, the health insurance and reinsurance industries must actively follow the progress of COVID-19 patients and provide solutions that correspond to patients’ needs, particularly related to the complications listed earlier.
Part 2: How is underwriting for the Life, Critical Illness, and Disability aspects of COVID-19 are evolving with developing medical knowledge?
As previously outlined, COVID-19 is turning out to be a highly intricate virus, combining the systemic consequences (Respiratory, Cardiovascular, Renal, Neurological, etc.) with related mental illness issues/risks. These multiple, potential, impacts on the health of a patient are presenting underwriters with unique challenges, beyond those faced in the industry before. This is especially the case as it relates to the continuing application of sound and fair underwriting decisions.
The far-reaching impact of COVID-19 extends beyond the virus itself to include macro consequences related to pre-COVID-19 healthcare services, economic impact, lifestyle changes, occupations, freedom of movement, and so on. All these factors are important to take into consideration in the underwriting of the various protection benefits that customers require.
As a global reinsurer, a fundamental part of SCOR’s purpose is to provide as much needed protection to as many people as possible. We therefore have a duty to the consumer to ensure we understand, monitor, and share the outcome of our learnings from our medical and knowledge expertise. Consumers are looking to protect themselves against future risk, and the current COVID-19 crisis provides an opportunity to deliver on our purpose. Overall, we will balance this macro-factor underwriting approach, with empathy, protection, and risk management. We will guide the best possible terms for a fair and evidence-based decision and offer the necessary protection to all the people we reinsure.
When COVID-19 first emerged, we took immediate steps to advise our clients on the underwriting of mortality and morbidity linked to multiple risk factors (co-morbidities). We then started to work on understanding the outcomes from the complications linked to COVID-19.
In addition to the medical information taken into consideration, as outlined previously, the underwriting process also takes into consideration the Case Fatality Rate (CFR) and Infection Fatality Rate (IFR). This adds to the complexity of underwriting as both CFR and IFR vary between countries and even down to the state, city, and region level within each country. These are also additional factors which influence our underwriting approach.
As we await the successful development of a vaccine as well as more effective methods of treating the consequences of COVID-19, it is fundamentally important that underwriting guidelines are agile enough to adapt to emerging knowledge concerning post-intensive care syndrome (PICS) and the other risk factors mentioned above. It is likewise important to closely follow the incidence mitigation policies put in place by governments leading to improved mortality and morbidity outcomes.
How we apply our philosophy based on the above
Obviously, each applicant is considered individually but our guidelines allow for terms to be offered at standard rates for non-hospitalized applicants following one month of full recovery and a return to normal activities.
For more complex cases arising from the consequences outlined previously, we categorize the severity of the COVID-19 sequalae and then apply terms according to this severity.
The definitions of severity are as follows:
Minor sequelae or complications, residuals and/or side-effects of treatment (non-exhaustive list):
- Dyspnoea
- Damage to vocal cords or dental
- Cutaneous damage such as bedsores
- Fatigue
- Difficulties with prolonged standing / walking
Mild to Moderate:
- Symptoms limited to flu-like symptoms, dry cough or fever
Severe:
- Pneumonia, Moderate-to-severe Dyspnoea
- Residual respiratory symptoms or Severe complications to COVID-19 may include significant lung damage, COPD, acute respiratory distress syndrome (ARDS), shock, myocarditis, arrhythmia, cerebral hypoxia or multiorgan dysfunction.
We constantly update SOLEM, our underwriting manual, to reflect the above input. For example, we consider the following criteria for applying underwriting decisions to Life, Income Protection and Critical Illness, for applicants with a history of COVID-19:
- Confirmed diagnosis, asymptomatic, or mild-to-moderate symptoms with or without hospitalization
- Confirmed diagnosis, severe symptoms with history of hospitalization or Intensive care Unit.Our info pages within the COVID-19 section of SOLEM also provide additional background to justify our approach.
For a full analysis, further information is available through SOLEM:
USA and Canada Rest of the world
In conclusion, the current unprecedented health crisis from COVID-19 will mark world history and will change our industry through challenges in underwriting and the adaptation of our risk management approaches. But it will also provide opportunities, such as in product development, and speed up the current technological and innovative underwriting evolution. We need to continue to grow and share our knowledge, to ensure we meet the challenge as an industry to prove our ability to understand, adapt and provide fair and justified underwriting decisions, and in turn provide the necessary protection to the consumer. The information provided above illustrates the complex nature of the medical sequalae (both physical, systemic and neuro-psychiatric) of COVID-19. It is fundamental that we, as a global reinsurer, along with the broader insurance industry, take the responsibility to ensure we provide the best possible advice and underwriting terms for the consumer.
As usual, at SCOR we remain available to assist our client partners with this ongoing challenge.
Resources
Ahmed, Hassaan, et al. "Long-term clinical outcomes in survivors of severe acute respiratory syndrome and Middle East respiratory syndrome coronavirus outbreaks after hospitalisation or ICU admission: a systematic review and meta-analysis." Journal of Rehabilitation Medicine 52.5 (2020).
B. Long, W.J. Brandy, A. Koyfman, et al., Cardiovascular complications in COVID-19, American Journal of Emergency Medicine, https://reader.elsevier.com/reader/sd/pii/S0735675720302771?token=43D99B02EF53685C2C73D9D7CEEE41385E2B5F411D047AA2F0BA9792814ACADCE8CFFED1901CA63DDF655F2E345C7498
Batlle, Daniel, et al. "Acute kidney injury in COVID-19: emerging evidence of a distinct pathophysiology." Journal of the American Society of Nephrology (2020).
Bikdeli, Behnood, et al. "COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review." Journal of the American College of Cardiology 75.23 (2020): 2950-2973.
Fox, Sharon E., et al. "Unexpected Features of Cardiac Pathology in COVID-19 Infection." Circulation (2020).
Herridge, Margaret S., et al. "Functional disability 5 years after acute respiratory distress syndrome." New England Journal of Medicine 364.14 (2011): 1293-1304.
Huang, Lu, et al. "Cardiac involvement in recovered COVID-19 patients identified by magnetic resonance imaging." JACC: Cardiovascular Imaging (2020).
Hong, Xia, et al. "Posttraumatic stress disorder in convalescent severe acute respiratory syndrome patients: a 4-year follow-up study." General Hospital Psychiatry 31.6 (2009): 546-554.
Lam, Marco Ho-Bun, et al. "Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: long-term follow-up." Archives of internal medicine 169.22 (2009): 2142-2147.
Lee, So Hee, et al. "Depression as a mediator of chronic fatigue and post-traumatic stress symptoms in middle east respiratory syndrome survivors." Psychiatry investigation 16.1 (2019): 59.
Nath, Avindra. "Neurologic complications of coronavirus infections." (2020).
Preiser, Jean-Charles, Margaret S. Herridge, and Elie Azoulay, eds. Post-Intensive Care Syndrome. Springer, 2020
Puntmann VO, Carerj ML, Wieters I, et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. Published online July 27, 2020. doi:10.1001/jamacardio.2020.3557
Wu, Xiaohua, Dawei Dong, and Daqing Ma. "Thin-section computed tomography manifestations during convalescence and long-term follow-up of patients with severe acute respiratory syndrome (SARS)." Medical science monitor: international medical journal of experimental and clinical research 22 (2016): 2793.
Zhang, P., Li, J., Liu, H. et al. Long-term bone and lung consequences associated with hospital-acquired severe acute respiratory syndrome: a 15-year follow-up from a prospective cohort study. Bone Res 8, 8 (2020). https://doi.org/10.1038/s41413-020-0084-5